
Why so many families are living with both diagnoses at once
Understanding the autism OCD difference same child situation is one of the most important clinical challenges facing families today. If your child has autism, you may have also heard the word OCD thrown around by therapists, psychiatrists, or teachers. Or maybe you have noticed behaviors that look like rituals, compulsions, or obsessive worry, and you are not sure if that is part of the autism or something separate entirely.
This is one of the most confusing areas in pediatric mental health, because autism and OCD overlap in so many visible ways. Both can involve repetitive behaviors. Both can involve intense focus on specific topics. Both can involve serious distress when routines are disrupted. (If you have ever wondered about the difference between a meltdown and an anxiety episode, this article on autism meltdown vs tantrum breaks down the differences in a way that is actually useful for moms.) But they are different conditions with different root causes and very different treatment approaches.
Getting this right matters. A lot. Because treating OCD in an autistic child as if it is just autism can leave real suffering unaddressed. And treating autistic behaviors as if they are OCD can backfire in ways that harm your child.
This article breaks down what is actually happening in each condition, how they look alike, how they differ, and what to do if you suspect your child has both.
What OCD actually is
Obsessive-compulsive disorder is an anxiety disorder. The core experience is this: an unwanted, intrusive thought or image pops into the mind (the obsession), and it causes intense anxiety or discomfort. To relieve that discomfort, the person performs a behavior (the compulsion). The compulsion works temporarily, which reinforces the cycle.
OCD is not about being neat or organized. It is about being trapped in a loop of fear and relief-seeking that the person does not want to be in. Children with OCD often know their fears are not rational. They may feel ashamed of their compulsions. They may try to hide them. The behaviors are driven by anxiety, not preference.
Common OCD themes in children include fear of contamination, fear of harm coming to a family member, religious fears, fear of being a bad person, and intrusive violent or sexual images. The compulsions can be visible (hand washing, checking, counting) or mental (repeating phrases silently, mentally reviewing events).
What repetitive behaviors in autism actually are
Repetitive behaviors in autism serve a completely different function. They are called restricted and repetitive behaviors, or RRBs, and they are a core feature of autism itself. They include:
- Stimming (self-stimulatory behavior) such as rocking, hand-flapping, spinning
- Insistence on sameness and rigid routines
- Highly specific, intense special interests
- Repetitive speech, scripting, echolalia
- Sensory-seeking or sensory-avoiding behaviors
These behaviors are typically not driven by anxiety about a feared outcome. They are driven by sensory regulation, enjoyment, comfort, or neurological difference. Many autistic people describe stimming as deeply pleasurable or calming, not something they are trying to escape.
The key distinction is ego-syntonic versus ego-dystonic. Autistic repetitive behaviors tend to be ego-syntonic, meaning the person accepts them as part of themselves. OCD compulsions are ego-dystonic: the person experiences them as alien, unwanted, distressing intrusions.
Where autism and OCD look identical from the outside
| What It Looks Like | When It Is Autism | When It Is OCD |
|---|---|---|
| Rigid routines | Deviation is distressing to the nervous system | Deviation triggers fear of specific harm |
| Checking behaviors | Symmetry and order feel important sensorially | Driven by fear that something bad will happen if the check is skipped |
| Touching or arranging objects | Sensory satisfaction in lining, sorting, or arranging | Arranging to prevent a feared catastrophe |
| Avoidance | Sensory overload or disrupted regulation | Fear of a specific outcome |
Here is where it gets complicated. Some behaviors look exactly the same whether the cause is autism or OCD:
Insistence on routines: An autistic child may need to follow the exact same bedtime sequence every night because deviation is distressing to their nervous system. A child with OCD may need to follow the exact same bedtime sequence to prevent feared harm. From the outside, both look like rigidity.
Checking behaviors: An autistic child might check that all the windows are closed because symmetry and order feel important to them. A child with OCD might check because they are terrified something bad will happen if they do not.
Touching or arranging objects: An autistic child might line up toys for sensory satisfaction. A child with OCD might arrange objects to prevent a feared catastrophe.
Avoidance: Both autism and OCD can produce intense avoidance of certain situations, people, or objects. The reason behind the avoidance is different, but the behavior looks the same.
The clinical difference that matters most
The most important clinical question is: what function is the behavior serving?
If the behavior is driven by an obsessional fear, if stopping it causes escalating anxiety around a feared outcome, and if the child experiences the behavior as something they do not want to do but feel they must, that points toward OCD.
If the behavior is driven by sensory needs, predictability preferences, or genuine enjoyment, if stopping it causes distress because of sensory overload or disrupted regulation (not fear of a specific outcome), and if the child experiences the behavior as natural and self-expressive, that points toward autism.
A skilled clinician will ask detailed questions about the antecedents to the behavior, the function of the behavior, and the child’s own experience of it. This requires an evaluator who understands both autism and OCD at a deep clinical level, which is still rare.
Why co-occurrence is common
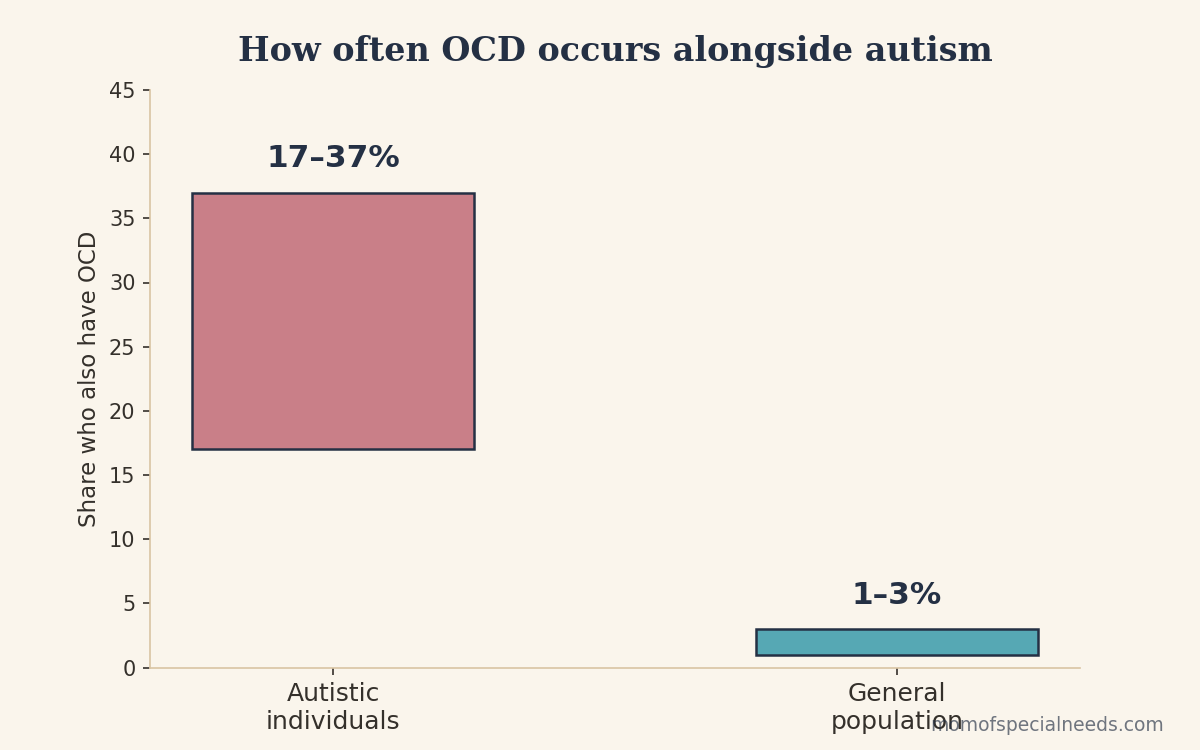
Research consistently shows that OCD is significantly more common in autistic people than in the general population. Estimates vary, but many studies suggest that somewhere between 17 and 37 percent of autistic people also meet criteria for OCD, compared to roughly 1 to 3 percent in the general population.
The reasons for this overlap are not fully understood, but several factors likely contribute. Autistic people experience higher baseline anxiety, which may make the OCD anxiety spiral more likely to take hold. Autistic people may also have differences in how they process uncertainty and predict outcomes, which are areas that overlap with OCD vulnerability. There may also be shared genetic and neurological factors that predispose individuals to both.
Why standard OCD treatment needs to be adapted for autism
The gold-standard treatment for OCD is exposure and response prevention, known as ERP. The idea is that the patient faces the feared situation without performing the compulsion, allows anxiety to peak and subside, and gradually learns that the feared outcome does not occur.
ERP works well in the general population. But for autistic children, it needs significant adaptation. Here is why:
First, the sensory differences and interoceptive challenges in autism mean that anxiety manifests differently, sometimes more intensely, and autistic children may have less ability to report what they are experiencing internally. Second, many ERP programs rely on verbal explanation and metaphor, which may not be accessible. Third, an autistic child may not have the same cognitive framework to understand the logic of ERP. Fourth, therapists need to be able to distinguish between an autistic child experiencing OCD distress during exposure versus an autistic child experiencing sensory overload or autistic burnout.
When navigating the autism OCD difference same child situations, a therapist who specializes in both conditions, or who works in close collaboration with an autism specialist, will produce far better outcomes than a therapist skilled in only one of these areas.
What this looks like for real families
You might see a child who has clear autism traits, communicates in their own way, loves their special interests, and also cannot leave the house without checking the door three times, because if they do not check, something terrible will happen to their mom. Or a child who arranges their toys a certain way for sensory pleasure and also cannot eat anything touching, because contamination feels like a true danger. Or a child who insists on routines for regulation and also needs to perform elaborate mental rituals to prevent feared harm that they cannot always articulate.
These children exist. They are in our community. And they deserve evaluation and treatment that addresses both conditions, not just one.
What parents can do when facing autism OCD difference same child challenges
If you suspect your child has OCD alongside their autism, here are concrete steps:
First, seek an evaluation from a psychologist or psychiatrist who has documented experience with both autism and OCD. Not just one. Both. This is not the time to see a general therapist who has read a little about autism. Ask specifically about their training in ERP and their caseload of autistic clients.
Second, document what you observe at home. Write down the specific behaviors you are seeing, when they happen, what seems to trigger them, whether your child seems distressed by them or comfortable with them, and whether they escalate when the child is anxious. This information is invaluable for a diagnostic assessment.
Third, do not try to eliminate repetitive behaviors without knowing their function. If the behavior is autistic stimming, suppressing it can cause harm. If it is OCD, treating it as stimming and ignoring it leaves the anxiety untreated.
Fourth, trust your gut. You know your child. If something feels different, if a behavior seems driven by fear rather than pleasure, if your child seems trapped rather than content, that is worth pursuing with a professional who can properly assess both conditions.
A note on diagnosis
Some children with autism also have an OCD diagnosis on their chart. Others have behaviors that fit OCD criteria but were never separately diagnosed because they were folded into the autism. Others are diagnosed with OCD first and their autism is missed entirely, which can lead to years of treatments that do not address the underlying neurology.
Understanding the autism OCD difference same child families navigate matters deeply. Accurate diagnosis matters not because labels define your child, but because the right label opens the door to the right interventions. If you are newer to the autism journey, this honest guide on what to do after an autism diagnosis can help you find your footing. If your child has both, they deserve both to be treated.
Frequently Asked Questions
Can a child have both autism and OCD at the same time?
Yes, and understanding the autism OCD difference same child families face is critical to getting the right help. Autism and OCD co-occur far more often than in the general population. Research suggests that between 17 and 37 percent of autistic individuals also meet criteria for OCD. Having autism and OCD simultaneously is a real and recognized clinical presentation that requires evaluation and treatment addressing both conditions.
How do I know if my autistic child’s repetitive behaviors are OCD or just autism?
The key question is function. Autistic repetitive behaviors typically serve a sensory or regulatory purpose and the child is generally comfortable with them. OCD compulsions are driven by anxiety about a feared outcome, and the child experiences them as unwanted and distressing. A psychologist with expertise in both conditions can help distinguish them through careful clinical assessment.
What is the best treatment for OCD in autistic children?
Exposure and response prevention, or ERP, is the evidence-based treatment for OCD, but it must be significantly adapted for autistic children. This requires a therapist with specific training in both ERP and autism, who can modify the approach to account for sensory differences, communication styles, and the unique way anxiety presents in autistic individuals.
Can OCD look like autism traits?
Yes, and this is one reason OCD is often missed in autistic children. The rigidity, checking, and repetitive behaviors of OCD can look identical to autistic insistence on sameness and repetitive behaviors from the outside. The distinction lies in the internal experience and function of the behavior, which requires careful clinical assessment to identify.
My child’s OCD behaviors seem to get worse when they are anxious overall. Is that normal?
Yes. OCD symptoms typically worsen under stress or increased anxiety. For autistic children, this can mean that OCD symptoms spike during sensory-intense environments, transitions, school stress, or any period of heightened anxiety. This interconnection is one reason addressing overall anxiety management is often part of treating OCD in autistic children.

